Article Notes
- Semi-rigid cup type (3M 1860 or 1860S): 65% FT pass.
- Duckbill type: (BSN ProShield or Halyard Fluidshield): 59% FT pass.
- Flat-fold cup type: (BYD Care DE2322): 32% FT pass.
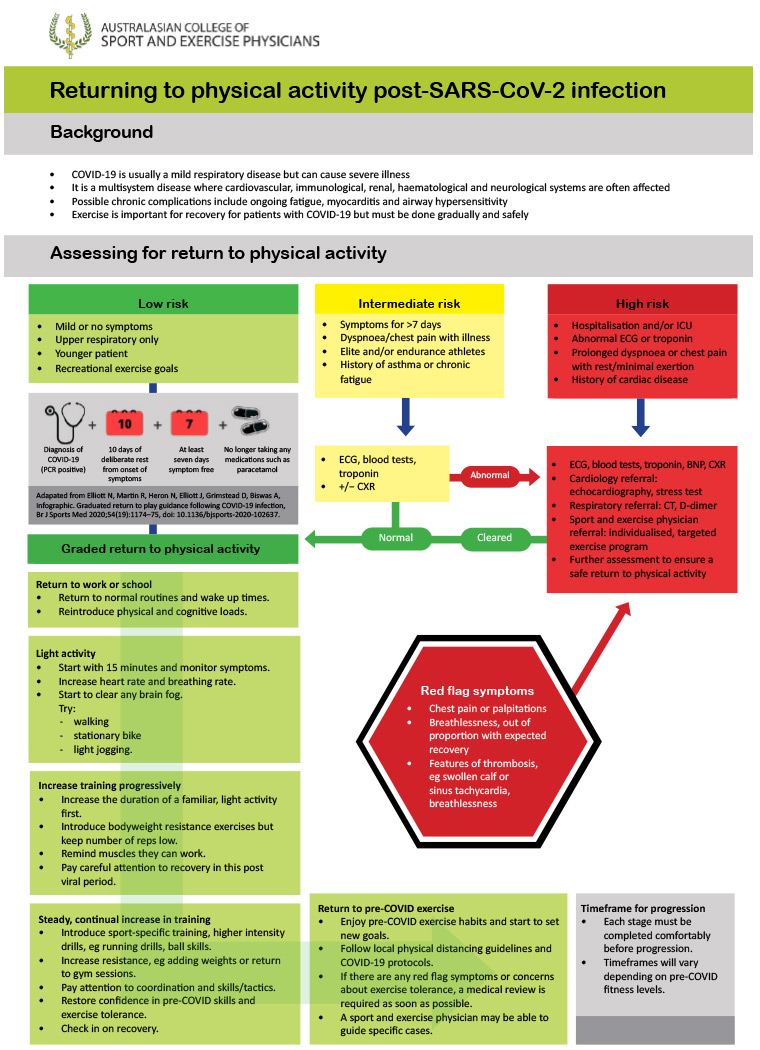
Low: Under 50 years with mild illness resolving within 7 days.
Intermediate: prolonged symptoms (>7d); persistent SOB or chest pain; pre-existing comorbidities; elite/endurance athletes.
- Consider ECG & baseline pathology, including troponin.
High: hospitalised with COVID; SOB or chest pain at rest; cardiac abnormalities.
- Multi-disciplinary team to advise & monitor return to exercise.
- Begin after 10 days of rest and when 7 days symptom-free.
- Begin with 15 minutes of light activity, with gradual increase guided by lack of fatigue with activity.
- 🚩Red flag symptoms: chest pain, palpitations, severe dyspnoea. STOP & medical review.
The usual 'correlation is not causation' qualifier is very necessary here. Perhaps doubly-so because this is a meta-analysis using pooled data of over 1 million people.
It's completely possible that someone who chooses to receive an influenza vaccine is also someone who makes more cautious health decisions and is more risk-averse, reducing their COVID exposure risk. The vaccinated are also more likely to be from better health-serviced locations and probably from higher socio-economic groups.
Still, interesting association nonetheless.
 Daniel Jolley
Daniel Jolley
Excellent audit data from a major Australian teaching hospital reporting on the fit test results of their tested 2,161 healthcare workers across four different N95/P2 mask designs.
Why is this important?
Many healthcare workers and significantly, the general public, do not have access to formal Fit Testing (requires expertise, facilities & equipment). We also know that as face shape varies among individuals, so does the effectiveness of protection for different mask types – this is particularly significant for women who have more difficulty in finding suitably-fitting N95 respirators. (Notably 73% of Fit Tested staff in this study were women.)
The results of this study may allow individuals to make educated choices on suitable masks even when they do not have access to Fit Testing, as well as guiding institutional mask purchases.
What did they find?
Three-panel flat-fold N95 masks performed best (3M Aura 9320A+) both for fit test (96% pass) and wearer comfort and usability.
The other three tested designs were not as performant:
Daniel Jolley
Jewson, McNamara & Fitzpatrick describe a roadmap for return to activity after COVID infection, developed by the Australasian College of Sport and Exercise Physicians.
They consider three risk categories:
Graded return to physical activity
Return to exercise flowchart:
Daniel Jolley
Early in the COVID pandemic, diagnostic testing relied entirely on precise-but-expensive PCR testing. Late in 2020 the Lateral Flow Testing techniques, already widely used for home-pregnancy tests and similar, were developed for SARS-CoV-2 antigens, leading to COVID-19 Rapid Antigen Tests (RATs).
While cheap, scalable and able to give a result in 10-15 minutes, they were initially seen mostly as a supplement to PCR testing, with less accuracy. Although true that RATs have lower sensitivity than SARS-CoV-2 PCR – most licensed-RATs have sensitivity 80-95% – today this is both less important, and possibly even a strength of RATs over PCR.
Early in the pandemic the role of testing has primarily about diagnosis, in those either symptomatic or pre-symptomatic. Viral presence was practically assumed to be synonymous with contagion. Today with over half a billion cumulative COVID cases worldwide and counting, along with access to effective vaccines and antivirals, it is often more useful to know whether an individual is infectious or not at a discrete moment in time.
Growing research over the last 12 months shows that adequately-sensitive RATs are effective at identifying infectious individuals, even if the high-sensitivity of PCR testing identifies viral particles in those who are infected but otherwise non-infectious (either pre-infectious, or post-infectious with ongoing viral shedding).
PCR positive results with cycle thresholds (ie. number of thermal cycles of RNA replication required before fluorescence is detected) above 25-30 have good correlation with being non-infectious (ie. unable to culture virus). Adequately approved & validated RATs (by FDA, TGA, MHRA, etc.) have very high sensitivity at CT less than this 25-30 range, depending on the study and specific manufacturer.
The bottom line...
An adequately-validated RAT, when correctly performed, is likely a sensitive indictor of individual infectiousness at that specific moment in time. The reliability of a negative RAT will be improved if using the same manufacturer and technique as a RAT previously positive test, and more so if there are several subsequent negative RATs.
Daniel Jolley
This study is primarily an evaluation of a specific RAT, the Coris coronavirus disease 2019 Ag Respi-Strip test – which while showing poor sensitivity, it again demonstrates that RAT-positivity correlates with viral load. This study used PCR-detection as the gold standard for evaluation, which because of the extreme sensitivity of PCR testing, does not easily translate to assessment of contagiousness (although Ct > 25-30 seems to correlate with inability to grow in viral culture).
Daniel Jolley
Early 2021 update of the 2020 Cochrane Review: Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection.
Better data is now available on correlation between PCR cycle threshold and likely infectivity.
Daniel Jolley
Although labelled as 'false' negative, negative RATs associated with positive PCR results, were in this study all in low viral-concentration patients, determined by a high PCR cycle threshold (ie. number of thermal cycles of RNA replication required before fluorescence is detected).
High PCR CT / calculated low-viral-concentration, correlates well with low/non-infectivity of the individual. This does not mean that they may not become infectious in the future, but rather means that at that point in time they are unlikely to be infectious.
Daniel Jolley
Early 2020 studies of COVID rapid antigen tests were of low quality and of variable applicability to COVID diagnostic decisions. This situation improved dramatically in 2021 and 2022, and many RATs are now continually validated in existing and emerging variants.
This Cochrane Review was updated in 2021.
Daniel Jolley
Van Decar et al. on the diagnosis and management of intra-operative diabetes insipidus concludes:
For the average adult patient, urine output >125 mL/h is consistent with polyuria. Urinary osmolality and specific gravity should be obtained and levels <300 mOsm/kg and <1.003, respectively, are consistent with hypotonic urine.
It is prudent to rule out other causes of polyuria including hyperglycemia, uremia, or iatrogenic causes including diuretic or mannitol administration.
Serum electrolytes and osmolality should also be obtained, and a high sodium (>146 mmol/L) and plasma osmolality (>300 mOsm/kg) are typically seen with DI.
Treatment should focus on replacement of free water deficit with a balanced salt solution, pharmacotherapy including DDAVP or vasopressin as appropriate, and close monitoring of patient’s fluid and electrolyte status.
Daniel Jolley