Article Notes
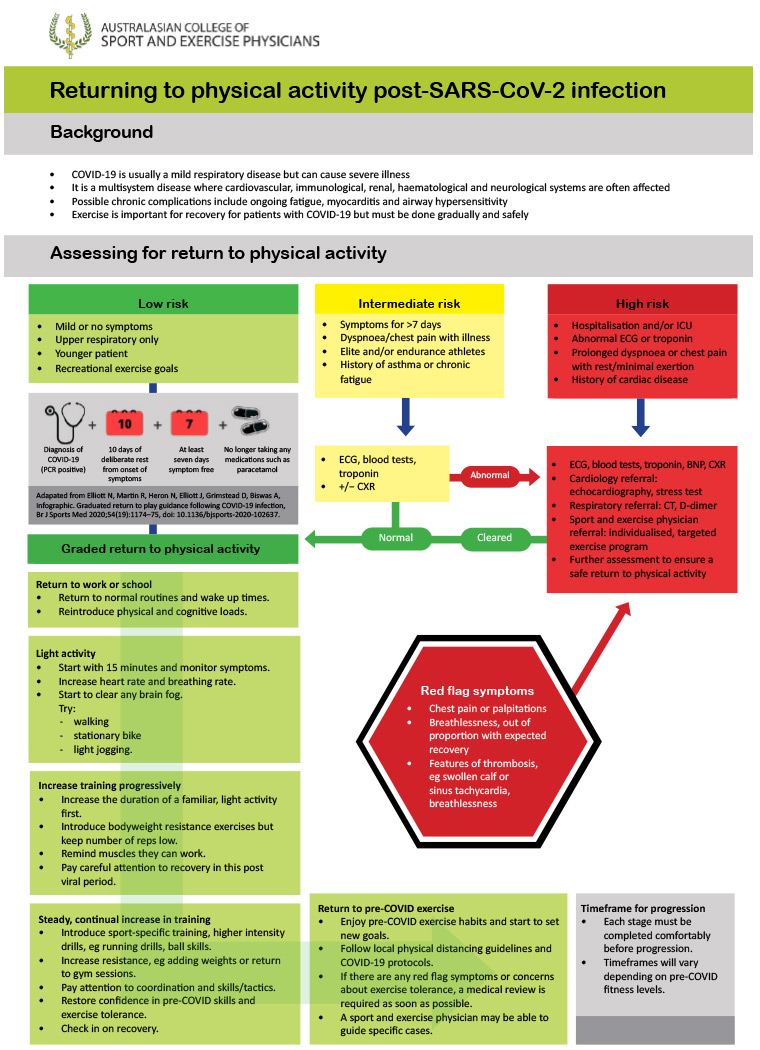
Low: Under 50 years with mild illness resolving within 7 days.
Intermediate: prolonged symptoms (>7d); persistent SOB or chest pain; pre-existing comorbidities; elite/endurance athletes.
- Consider ECG & baseline pathology, including troponin.
High: hospitalised with COVID; SOB or chest pain at rest; cardiac abnormalities.
- Multi-disciplinary team to advise & monitor return to exercise.
- Begin after 10 days of rest and when 7 days symptom-free.
- Begin with 15 minutes of light activity, with gradual increase guided by lack of fatigue with activity.
- 🚩Red flag symptoms: chest pain, palpitations, severe dyspnoea. STOP & medical review.
Jewson, McNamara & Fitzpatrick describe a roadmap for return to activity after COVID infection, developed by the Australasian College of Sport and Exercise Physicians.
They consider three risk categories:
Graded return to physical activity
Return to exercise flowchart:
 Daniel Jolley
Daniel Jolley
Early in the COVID pandemic, diagnostic testing relied entirely on precise-but-expensive PCR testing. Late in 2020 the Lateral Flow Testing techniques, already widely used for home-pregnancy tests and similar, were developed for SARS-CoV-2 antigens, leading to COVID-19 Rapid Antigen Tests (RATs).
While cheap, scalable and able to give a result in 10-15 minutes, they were initially seen mostly as a supplement to PCR testing, with less accuracy. Although true that RATs have lower sensitivity than SARS-CoV-2 PCR – most licensed-RATs have sensitivity 80-95% – today this is both less important, and possibly even a strength of RATs over PCR.
Early in the pandemic the role of testing has primarily about diagnosis, in those either symptomatic or pre-symptomatic. Viral presence was practically assumed to be synonymous with contagion. Today with over half a billion cumulative COVID cases worldwide and counting, along with access to effective vaccines and antivirals, it is often more useful to know whether an individual is infectious or not at a discrete moment in time.
Growing research over the last 12 months shows that adequately-sensitive RATs are effective at identifying infectious individuals, even if the high-sensitivity of PCR testing identifies viral particles in those who are infected but otherwise non-infectious (either pre-infectious, or post-infectious with ongoing viral shedding).
PCR positive results with cycle thresholds (ie. number of thermal cycles of RNA replication required before fluorescence is detected) above 25-30 have good correlation with being non-infectious (ie. unable to culture virus). Adequately approved & validated RATs (by FDA, TGA, MHRA, etc.) have very high sensitivity at CT less than this 25-30 range, depending on the study and specific manufacturer.
The bottom line...
An adequately-validated RAT, when correctly performed, is likely a sensitive indictor of individual infectiousness at that specific moment in time. The reliability of a negative RAT will be improved if using the same manufacturer and technique as a RAT previously positive test, and more so if there are several subsequent negative RATs.
Daniel Jolley
This study is primarily an evaluation of a specific RAT, the Coris coronavirus disease 2019 Ag Respi-Strip test – which while showing poor sensitivity, it again demonstrates that RAT-positivity correlates with viral load. This study used PCR-detection as the gold standard for evaluation, which because of the extreme sensitivity of PCR testing, does not easily translate to assessment of contagiousness (although Ct > 25-30 seems to correlate with inability to grow in viral culture).
Daniel Jolley
Early 2021 update of the 2020 Cochrane Review: Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection.
Better data is now available on correlation between PCR cycle threshold and likely infectivity.
Daniel Jolley