Article Notes
- Hospitals are frequent sources of outbreaks, among both staff, patients and the wider community.
- The quality of PPE evidence is low. Most evidence must be contextualised in consideration of expert opinion, and of the similarities between SARS-CoV-2 and SARS (SARS-CoV-1), MERS and influenza.
- Droplet-vs-airborne spread is a conceptual simplification and not a simple dichotomy. It is best understood as a spectrum of transmission risk.
- Time-exposed may be a more important consideration, especially in indoor, poorly ventilated spaces.
- PPE supply is globally limited, and so a pragmatic approach must be taken to its use, considering individual risk scenarios.
- Training, simulation and fit testing are critical for effective use of PPE.
- There are specific steps in the PPE donning & doffing workflow that are frequently associated with breaches exposing HCWs to infection. These require extra attention.
- Beyond cost, increasingly complex PPE (eg. PAPR, hoods, intubation boxes etc.) also increase the opportunity for PPE failure and exposure if users have not had adequate training in their use, and some PPE has been demonstrated to make intubation more difficult.
- The superiority of N95/P2 respirator masks over standard surgical masks for personal protection is unclear and unproven.
- N95 mask fit-testing and fit-checking; notably shaving facial hair to ensure a face-mask interface seal.
- Use of extended-cuff gloves with gown cuff tucked securely into glove.
- Time management: PPE donning should never be rushed, even in critical medical emergencies.
- Glove removal is a high-risk step. When removing the second, inner glove, ensure as little contact as possible with the glove sleeve by the ungloved hand.
- Gown removal is the next highest risk step. Do not touch the front of the gown, especially with ungloved hands.
- Mask removal avoid touching front of mask; avoid any snapping of straps.
- Perform alcohol-based hand-hygiene after each article is removed.
- Powered air-purifying respirator (PAPR) with coverall may be more protective than N95 masks and gown (RR 0.27), but create unique donning challenges.
- Long-gowns may be better than a coverall, but are also more difficult to doff. Gowns are better than aprons. Better sealing, fitting, and one-piece removal at gown-glove interfaces and closer fit around the neck may reduce exposure.
- Double-gloving may reduce exposure.
- Better training, computer simulation, video lectures, following CDC protocols, and spoken instruction may improve donning and doffing compliance.
- Laryngeal activity - talking, coughing, sneezing.
- High velocity gas flow - eg. high-flow oxygen
- Cyclical opening & closing of terminal airways.
- Despite this history we remain unprepared for a pandemic.
- From an ICU perspective, conservative models predict >170% ICU resource utilisation due to a pandemic. They note that most health systems would struggle with even this optimistic surge.
- SARS experience in Canada, despite only 251 cases, critically stretched hospital and ICU resources.
- Pandemic surveillance.
- Prepare health-system scalability to manage surge: equipment, physical space, human resources, and system (eg. stepped triage plans).
- Prepare for mass vaccine production.
- Better coordinate and integrate communications.
- Streamlined research and ethics proposals for rapid initiation.
Public Health England's 'New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG)' concluded:
It is biologically plausible that chest compressions could generate an aerosol, but only in the same way that an exhalation breath would do. No other mechanism exists to generate an aerosol other than compressing the chest and an expiration breath, much like a cough, is not currently recognised as a high-risk event or an AGP.” NERVTAG also stated that it “does not consider that the evidence supports chest compressions or defibrillation being procedures that are associated with a significantly increased risk of transmission of acute respiratory infections.”
 Daniel Jolley
Daniel Jolley
Also worth considering, is the impact that CPR and external compressions may have on undermining the effective protection of PPE, given that CPR is a uniquely dynamic and physical activity compared to most medical procedures.
Using simulation studies, Hwang et al. have already brought into question the effectiveness of N95 masks during CPR:
N95 respirator masks may not provide adequate protection during chest compressions, even when resuscitators have passed quantitative fit testing.
Daniel Jolley
Some of the assertions in this review are challengable, and based upon sources with lesser certainty than suggested. For example:
"COVID-19 is predominantly caused by contact or droplet transmission..." - Cook
Yet the reference for this is a Public Health England statement describing this as an 'assumption' without evidence. In contrast there is now considerable debate as to the significance of airborne COVID-19 transmission.
"The transmission of COVID-19 is thought to occur mainly through respiratory droplets generated by coughing and sneezing, and through contact with contaminated surfaces. The predominant modes of transmission are assumed to be droplet and contact." – Public Health England
Because PPE recommendations are based upon this assumption, caution is still required.
Daniel Jolley
This growing collection of articles focuses on the evidence and expert guidance relating to the use of personal protective equipment (PPE) and the SARS-CoV-2 / COVID pandemic, with specific focus on PPE use by anaesthesiologists and anaesthetists.
More articles can found found via the PPE topic index.
What we know:
Daniel Jolley
Toronto anaesthesiologists Muñoz-Leyva & Niazi share observations from PPE training simulations, identifying the 'high risk' moments where frequent exposures and PPE failures are seen.
Why is this important?
For all the understandable concern over adequate access to PPE and discussion of appropriate levels of protection, HCW safety is entirely dependent on the effective use of this protective equipment.
Identifying common areas of 'biosafety breach' allows both clinicians and PPE supervisors to apply added attention to these steps. These areas can be conceptualised as offering a disproportionate safety benefit for the time and resources deployed in ensuring compliance at these moments.
Which areas did they identify as most important?
Donning
Doffing
Daniel Jolley
This relatively small study (N=19) randomised emergency resident trainees (14) and first responders (5) to cadaveric intubation with and without 'Level C PPE':
Level C PPE typically includes a full face mask with air respirator, a hooded chemical resistant clothing, inner and outer gloves and chemical resistant boots with covers.
First-pass intubation success was significant lower (58% vs 96%) while wearing PPE than without. Subjects identified the visibility impact of wearing protective hoods as the most common impediment to intubation.
Daniel Jolley
This is the second update to Verbeek et al.'s 2016 Cochrane Review of personal protective equipment (PPE) for preventing infections in healthcare workers (HCW). The prior update was in July 2019.
What's worth knowing?
Overall most studies of PPE efficacy are of low quality and offer a low certainty of conclusions. Caveat emptor...
Daniel Jolley
In this review, Wilson, Norton, Young & Collins challenge the overly-simplistic view that SARS-CoV-2 transmission risk can be easily divided between droplet-contact and aerosol precautions.
Why is this important?
Many national societies have policies on Personal Protective Equipment (PPE) guided by classification of COVID exposure into aerosol-generation procedures (AGP) or other exposures. Although founded in some evidence, there are questions as to whether PPE shortage and availability also drives these recommendations. Widespread concern over healthcare worker (HCW) infection is understandable, given that during SARS 20% of infections were among HCWs.
Understanding the science behind respiratory particle generation and transmission helps to inform our understanding of how best to use limited PPE.
On the science of respiratory shedding
Aerosol generation is important because virus inhalation and deposition in small distal airways may be associated with greater infection risk and disease severity. Wilson et al. describe three mechanisms of aerosol generation:
Notably, the clinically features of COVID itself make all three high-risk mechanisms more likely. Additionally various studies show that even talking and tidal volume breathing produce large numbers and size ranges of respiratory droplets.
Exposure relative risk is primarily about proximity and exposure duration
Further, considering retrospective data form SARS HCW infections involving various procedures (eg. intubation, HCW infection RR 4.2; oxygen mask manipulation RR 9; urinary catheterisation RR 5), Wilson et al. propose that healthcare work risk can be considered:
infection risk ∝ 𝑏 × 𝑣 × 𝑡 / 𝑒
Where: 𝑏 = breathing zone particle viable virion aerosol concentration, 𝑣 = minute volume of healthcare worker, 𝑡 = time exposed , 𝑒 = mask efficiency
And on intubation:
"...[other] healthcare workers should stand over 2 m away and out of the direct exhalation plume. During a rapid sequence intubation muscle relaxation should be protective as coughing will be prevented and high airway gas flow and expiratory output will terminate. When expiratory flow is ended ... aerosol particles should start settling in the airways. The forces generated in gentle laryngoscopy are unlikely to cause aerosol formation."
"...[there is] limited evidence to suggest AGPs cause an increase in airborne healthcare worker transmission as this has not been studied. The few studies to sample pathogenic airborne particles in relation to procedures show no increase with the majority of AGPs."
Bear in mind...
Much of the evidence guiding our understanding of SARS-CoV-2 transmission is founded on understanding and research focusing on the 2003 SARS pandemic (SARS-CoV-1) and influenza research. Although sharing similarities, "...each has its own infective inoculum and aerosol characteristics."
What's the bottom-line?
Transmission of SARS-CoV-2 should be conceptualised as a spectrum of risk where time exposed may be the dominant factor and droplet-airborne spread is a complex continuum of varying probability of infection. Many 'non-AGP' events could in fact be higher risk than those traditionally considered AGP, such as intubation.
Daniel Jolley
What is this?
Kain & Fowler's prescient review from October 2019 sets out how intensive care units should prepare and respond to the next pandemic, both practically at a hospital level and at a wider health-system. Although the focus was on an influenza pandemic, the advice is readily applicable to the SARS-COV-2 pandemic.
Background
They note that not only have we seen regular influenza outbreaks in addition to other viral pandemics, that due to increased urbanisation, population density, global travel and living proximity to animals, there is rapidly increasing global risk of a viral pandemic.
"When considering preparation for the next pandemic, it is not a matter of if it will occur, but rather a matter of when." – Kain & Fowler
They provide an overview of historical influenza pandemics over the last century, most recently with the 2009 H1N1 swine-flu pandemic, killing 300,000 people.
What preparation do they recommend?
Kain and Fowler suggest global focus on:
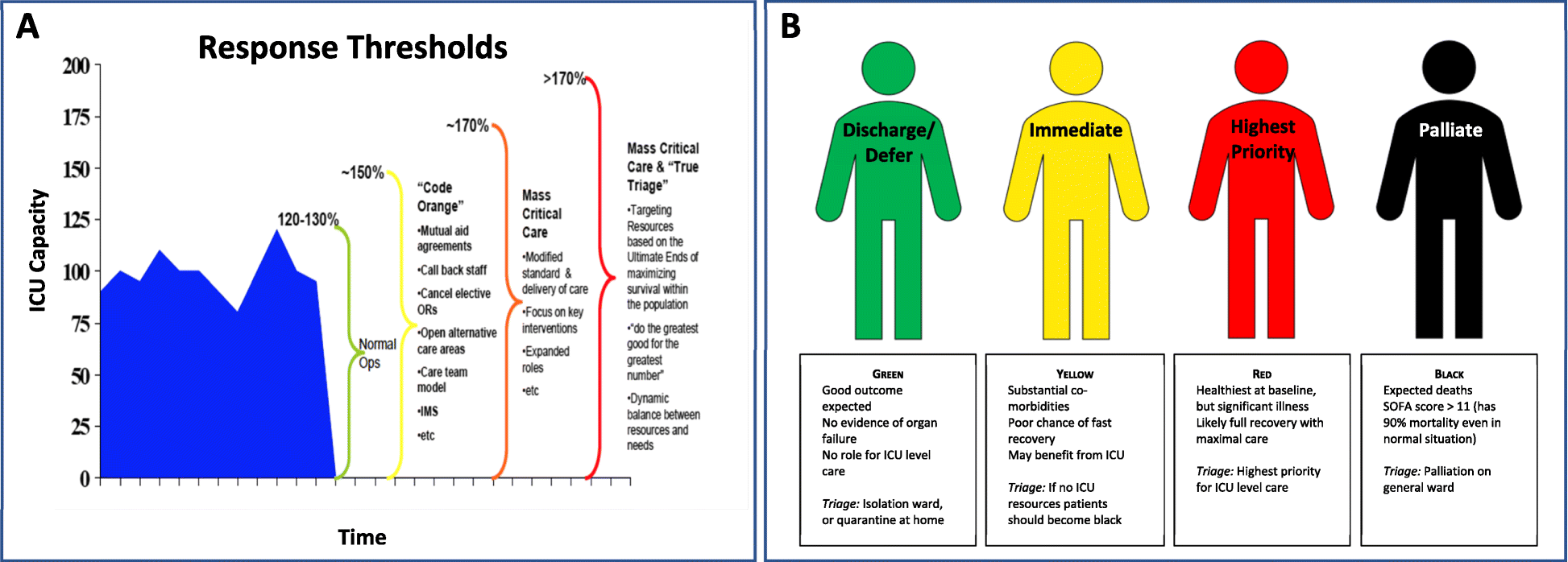
They highlight the importance of intensivists being involved in strategic planning, so as to coordinate ICU responses for "...triage, clinical care, and infection control." – noting that during SARS 20% of infections were in healthcare workers, and hospitals themselves became important sources of transmission.
Final word...
The IHR Committee's review following the 2009 H1N1 pandemic is now only too obvious:
“...the world is ill-prepared to respond to a severe influenza pandemic or to any similarly global, sustained, and threatening public-health emergency.” – International Health Regulations Committee (2011)
Daniel Jolley