Article Notes
- Semi-rigid cup type (3M 1860 or 1860S): 65% FT pass.
- Duckbill type: (BSN ProShield or Halyard Fluidshield): 59% FT pass.
- Flat-fold cup type: (BYD Care DE2322): 32% FT pass.
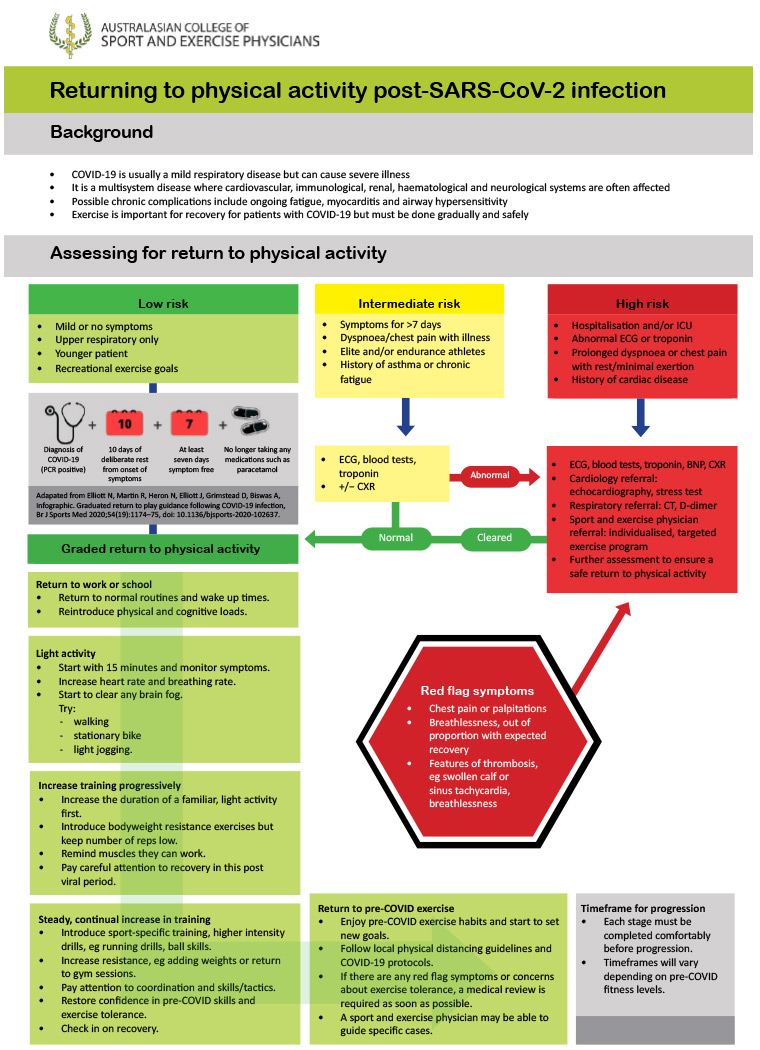
Low: Under 50 years with mild illness resolving within 7 days.
Intermediate: prolonged symptoms (>7d); persistent SOB or chest pain; pre-existing comorbidities; elite/endurance athletes.
- Consider ECG & baseline pathology, including troponin.
High: hospitalised with COVID; SOB or chest pain at rest; cardiac abnormalities.
- Multi-disciplinary team to advise & monitor return to exercise.
- Begin after 10 days of rest and when 7 days symptom-free.
- Begin with 15 minutes of light activity, with gradual increase guided by lack of fatigue with activity.
- 🚩Red flag symptoms: chest pain, palpitations, severe dyspnoea. STOP & medical review.
The usual 'correlation is not causation' qualifier is very necessary here. Perhaps doubly-so because this is a meta-analysis using pooled data of over 1 million people.
It's completely possible that someone who chooses to receive an influenza vaccine is also someone who makes more cautious health decisions and is more risk-averse, reducing their COVID exposure risk. The vaccinated are also more likely to be from better health-serviced locations and probably from higher socio-economic groups.
Still, interesting association nonetheless.
 Daniel Jolley
Daniel Jolley
Excellent audit data from a major Australian teaching hospital reporting on the fit test results of their tested 2,161 healthcare workers across four different N95/P2 mask designs.
Why is this important?
Many healthcare workers and significantly, the general public, do not have access to formal Fit Testing (requires expertise, facilities & equipment). We also know that as face shape varies among individuals, so does the effectiveness of protection for different mask types – this is particularly significant for women who have more difficulty in finding suitably-fitting N95 respirators. (Notably 73% of Fit Tested staff in this study were women.)
The results of this study may allow individuals to make educated choices on suitable masks even when they do not have access to Fit Testing, as well as guiding institutional mask purchases.
What did they find?
Three-panel flat-fold N95 masks performed best (3M Aura 9320A+) both for fit test (96% pass) and wearer comfort and usability.
The other three tested designs were not as performant:
Daniel Jolley
Jewson, McNamara & Fitzpatrick describe a roadmap for return to activity after COVID infection, developed by the Australasian College of Sport and Exercise Physicians.
They consider three risk categories:
Graded return to physical activity
Return to exercise flowchart:
Daniel Jolley